
Review Article | DOI: https://doi.org/10.31579/2690-8794/040
1 Department of Public and community Health, Novena University Ogume, Nigeria.
2 School of Community Health, Charles Sturt University, New South Wales, Australia
*Corresponding Author: Ezekiel Uba Nwose. Department of Public and Community Health, Novena University Ogume, Nigeria.
Citation: Orove A.A, Garba A, Orru M.O, Otovwe A, Igumbor E.O. and Nwose E.U., (2020) Gestational diabetes management postpartum in primary healthcare facilities: Mini review update on Delta State Nigeria; Clinical Medical Reviews and Reports, 2(7); DOI: 10.31579/2690-8794/040
Copyright: © 2020, Nwose E.U., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 August 2020 | Accepted: 26 August 2020 | Published: 09 September 2020
Keywords: behavioral change wheel; central hub role; gestational diabetes; postpartum follow up; primary healthcare; delta state nigeria
In this piece of the series on primary health care (PHC) as a ‘central hub’ role in health systems of Delta State Nigeria, focus is on gestational diabetes screening and postpartum follow up. Antenatal services offered by the governmental health system are rarely available in PHC facilities. Based on preliminary reports from ongoing studies, this narrative review articulates the potential of PHC to offer antenatal services including gestational diabetes screening and postpartum follow up. The basic evidence and need to enhance behavioural change wheel among all stakeholders, including but not limited to both the healthcare providers and community members, are presented.
Gestational diabetes (GDM) is considered a risk factor developing type 2 diabetes mellitus [1]. Recognition of this predisposition to diabetes and the significant population attributable to risk of GDM may provide opportunity and incentive to women with prior GDM to undertake lifestyle measures to reduce their diabetes risk. Models of screening for diabetes has also been a discussion point [2-4], because of the need of early identification and intervention. There is no gain saying the fact that substantial population health impact is possible through preventive strategies directed at women with prior GDM.
Debate has been ongoing for over a decade regarding the best model for GDM screening [5-7]. Notable among the models are the American Congress of Obstetricians and Gynecologists (ACOG), European Association for the Study of Diabetes (EASD) , Hyperglycemia and Adverse Pregnancy Outcomes (HAPO), International Association of Diabetes and Pregnancy Study Groups (IADPSG), and National Diabetes Data Group (NDDG) to mention a few. Major differences has been the number of steps such as two-steps of American Diabetes Association and NDDG and one-step of IADPSG and World Health Organization (WHO) [8]. Associated with these difference models is the concern of either over-diagnosis with potential impact on healthcare finances [4, 8], or under-diagnosis that may leave some GDM cases being missed [2, 3]. Not the least is also the divided opinions regarding selective versus universal screening. There are argument for and against each method, especially with regards to selective vs. universal screening [2, 3, 9, 10]. Therefore, it is worth acknowledging the fact that a plethora of models have caused lack of consensus.
Nevertheless, the issue of GDM care vis-à-vis screening and postpartum follow up is not completely that of laboratory methodology. Hence, this narrative is not joining the argument, but acknowledges the fact that there are pros and cons for any model or policy [2]. Importantly, this narrative focuses on acknowledged key issue that GDM is often undetected for reasons that can be easily avoided [11]. Hence, given the knowledge of risk factors for selective screening [2, 3], especially considering that such risk assessment are generally non-invasive and can be obtained during ANC registration and history taking [12-14], the agenda is to evaluate the capacity of GDM management postpartum in PHC facilities of Delta State Nigeria.
This narrative review was a progression of ongoing studies and started from preliminary evaluations’ data that have been previously published [15-19]. There were separate two clinical audits done at secondary and tertiary health facilities in the state [18, 19]; plus one expository review [16]. This narrative being a progression of the work attempts to bring all the findings in terms of capacity of the PHC facilities to screen and manage GDM. Two other journal articles that were discretionally selected and reviewed to support the discourse on knowledge attitude and practice (KAP) translated to behavioural change wheel (BCW).
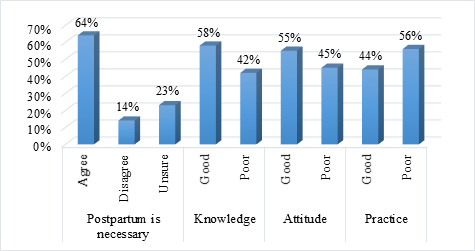
Healthcare providers’ evaluation: In the evaluation of diabetes care in Delta State, key findings included lack of endocrinologist, Diabetes Educator or register of referrals. Perceptions among the healthcare workers may be okay (Figure 1), but there is room for improvement [16]. In clinical audits, there is knowledge of appropriate test methods and opportunity to carry out the tests. What is generally lacking is motivation, which the healthcare workers attribute to patients behavior as well as the very low level of positive results. Major findings attributable to healthcare providers’ lack of expert service include

The evidence of knowledge and practice gap about postpartum management is indicated in the systematic review report of Utz et al [20]. According the report, three out of 23 studies identified postpartum practice, and this included one of the three studies from Nigeria. In another study that evaluated the KAP of doctors and nurses, a total of 34% either disagreed or were unsure that postpartum follow up is necessary. The report also indicated that while knowledge and attitude appear a little more, poor practice was higher (Figure 2). This report is in agreement with our previous report that the healthcare providers including ministry of health, hospital management board and the frontline staff healthcare professionals have capacities but poor in practice [15, 21].
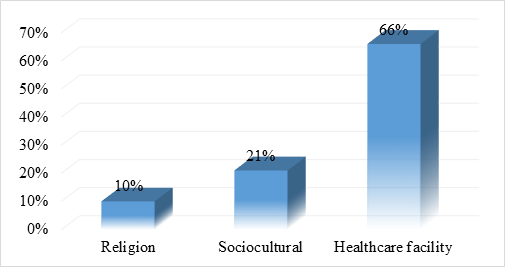
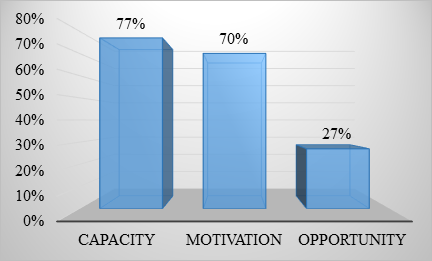
Community members’ evaluation: Observations from a survey further indicated barriers to diabetes care among the people to include lack of necessary knowledge and poverty [20]. However, more of the healthcare providers admitted that healthcare facility is the major militating factor relative to religion and sociocultural practice (Figure 3). In one of the reported surveys from preliminary studies [15, 21], 77% of the respondents did agree that patients in the community have poor capacity while 73% believe that the opportunity is there (Figure 4).
In clinical practice, there is KAP gap among antenatal service providers with regard to selective screening as well as concerted effort to diagnose GDM. There is also problem of postpartum GDM follow-up, which necessitates adoption of registry. While lack of diagnosis is sometimes attributed to cost of mass screening, it needs to be advocated in healthcare professionals and public health managers that there are GDM risk factors that can be assessed non-invasively to select patients for screening [12-14]. Further, both antepartum prediabetes and GDM are predictors of postpartum T2DM [22, 23]. This highlight has become necessary because the inconsistency of recording these data across the tiers of healthcare delivery in Nigeria is worrisome as indicated in recent report [24].
It is already established that the screening for GDM is uppermost if it must be dealt with. This is because GDM is asymptomatic and a large percentage of women of reproductive age have no classic risk factors, thus debate regarding the preferred screening protocol for GDM. Some experts
recommend universal screening because not all women who develop GDM have risk factors. The ADA policy states that screening may be omitted in low-risk women. A woman is considered low risk if all of the following factors are present: age younger than 25 years; BMI less than 25 before pregnancy; no first-degree relative with DM; no history of abnormal glucose tolerance; and no history of poor obstetric outcome among others. The ACOG practice bulletin states that universal screening is the most sensitive and more practical approach, but it notes that low-risk women may be excluded from screening per the ADA recommendation [25].
Ultimately, screening of GDM could be performed to the whole obstetric population (universal screening) or targeted at the high risk groups (risk factor screening). In the summary recommendations of the Fourth International Workshop Conference in 1997, risk factor screening was recommended and the statement was reaffirmed at the Fifth International Workshop Conference in 2005 [26]. When the universal screening approach is employed, patients with no known risk factors should undergo a 1-hour glucose test (glucose challenge test) at 24 to 28 weeks of gestation.
It is worthy of note that it has become worrisome in some part of developing countries were they do practice selective screening, which ultimately could be attributed to resource-deficient low-mid income countries such as Nigeria. In some instances, the selection is based on patient’s ability to pay for the screening test [18]. Whether this practice improves the level of patients identified with GDM is of interest to investigate. This opinion clearly lend more credence to the argument of Berger and Sermen [3], that in order to treat GDM, one must first screen for it. Ideally, the chosen screening protocol should identify subjects at maximal risk of adverse pregnancy outcomes who would most benefit from intensified management and surveillance, while freeing the rest from the burden of excessive interventions. Unfortunately, the policy of universal or near-universal screening that is recommended by numerous professional medical organizations will lead to the blanket labeling of a large group of women as having GDM, without differentiating between those at high and those at low risk of pregnancy complications. It has very clearly been shown that glucose intolerance in pregnancy is not a threshold phenomenon but, rather, is linked to several adverse pregnancy outcomes along a continuum of measured glucose values [9].
Benefits of screening is an agreeable diction. Screening for GDM and its consequent diagnosis can successfully lead to interventions that are likely to reduce the incidence of macrosomia while possibly increasing the CS rate. Reduction of macrosomia is only an intermediate endpoint, with reduction of birth trauma and possibly neonatal metabolic disorders being the true goal of GDM diagnosis and treatment [1, 18, 22, 23]. Evidence of other health benefits for the child or mother is not lacking [1], and this can be further picked up from the risk assessment and screening algorithm [4, 9, 10, 20]. In particular, preterm delivery is known [27], which absolutely impacts on the health of a child.
Among other benefits of screening and early intervention, reduction in perinatal mortality is one. Although an increase in perinatal mortality in women was said to be correlated with increase in GDM, studies have not been able to confirm this finding. One major reason for lack of justification is dearth of registries [18]. The overall decrease in perinatal mortality in recent years means that studies now require very large sample sizes in order to have the power to show an association between GDM and perinatal mortality [27]. Thus fetal deaths due to unrecognized GDM could go unnoticed in smaller studies.
Benefits of postpartum management is quite known including but not limited to prevention of the long-term effects of GDM on both the child and the mother. For instance, it had been highlighted that 40% of women living with diabetes are within reproductive age. About half of GDM cases progress to type 2 diabetes. The seriousness of these necessitated GDM being the theme of World Diabetes Day of 2017 [1]. What this narrative highlights is that PHC facilities can offer these services if the BCW is enhanced.
GDM is a problem that affects a significant number of women during pregnancy. GDM can have lasting health impacts on both the mother and child. In order to minimize potential complications, early diagnosis and intervention are critical. There is still work to be done to gain a better sense of what screening protocols are most efficacious and cost effective, and when they should be administered. Prevention of GDM at the Pre-GDM stage appears to be the focus of research. While this is well known, what is emphasized here is the KAP gap among healthcare providers. There is perception of poor practice in GDM services and also poor capacity in the patients. Yet, PHC facilities are capable of offering these services if given the necessary motivation and supervision to do so.
This piece of narrative is a collaborative work of three ongoing postgraduate research scholars in the department of Public and Community Health at Novena University.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
